Key takeaway: Diverticulitis treatment has changed a lot in recent years. In the past, nearly everyone with diverticulitis was treated with antibiotics, and surgery was recommended after one to two diverticulitis episodes. Thanks to evolving research, care is now more individualized and based on severity and personal risk. Antibiotics are no longer prescribed to most people with uncomplicated diverticulitis, and surgery is now recommended on a selective basis.
Diverticulitis treatment has gone through a makeover of sorts in recent years. Let’s just say, it’s not the same treatment protocol that your grandparents’ or even parents’ generations might remember.
Before we dive into the details, let’s do a quick review of diverticulitis and who even has it. To understand diverticulitis, you also have to understand diverticulosis. Up to 70% of people in Western countries are diagnosed with diverticulosis by the age of 80. But diverticulosis is quite different from diverticulitis. Diverticulosis is when you develop out-pockets in your intestinal walls (these are called diverticula), and it usually doesn’t cause any symptoms. Diverticulitis is where things get uncomfy: this is an inflammation or infection of the diverticula, which comes with symptoms like pain or diarrhea, and a whole host of potential complications.
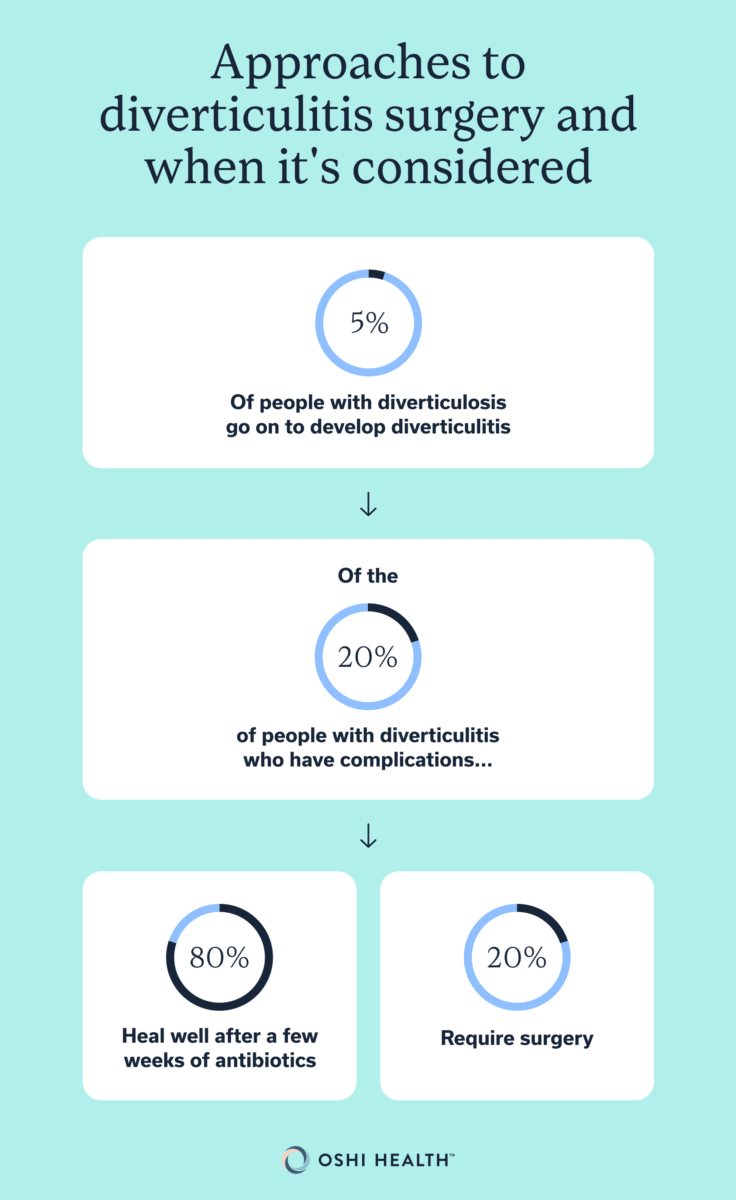
The good news is that only 5 percent of people with diverticulosis go on to develop diverticulitis. The bad news? This is still a pretty large group of people, since so many have diverticulosis to start with.
Treatment for diverticulitis used to be pretty straightforward, but it wasn’t exactly evidence-based: antibiotics for all, and routine surgery for those who had a certain number of recurrences. Thankfully, research in this area is growing, and diverticulitis care is now more individualized and less invasive. Here’s the lowdown on new treatments for diverticulitis, who gets antibiotics and surgery, what you’re allowed to eat, and prevention strategies.
New treatments for diverticulitis: What’s changed (and why)?
“Over the past 15 to 20 years, the management of diverticulitis has generally become less aggressive,” says Lisa Strate, MD, professor of medicine and chief of the Division of Gastroenterology and Hepatology at the University of Wisconsin School of Medicine and Public Health, who specializes in diverticulitis.
More people are now treated medically rather than surgically, and may not ever need to step foot in a hospital setting. Instead of a blanket recommendation of antibiotics, clinicians are more selective in prescribing. These days, most people with uncomplicated diverticulitis won’t have to take antibiotics. Surgery is also recommended less frequently, and given based on evidence-based risk and patient preference, rather than an arbitrary number of episodes.
There’s also an increased focus on preventing diverticulitis through lifestyle changes like diet and exercise. The old instruction to avoid nuts, seeds, and popcorn has also been replaced with more evidence-based advice to eat a diet rich in whole foods.
First step: Confirm what you’re dealing with (uncomplicated vs complicated)
The first step to treating diverticulitis is to figure out what kind of diverticulitis you’re dealing with. This is usually done with a computed tomography (CT) scan of your abdomen (which is a specialized X-ray that creates detailed images of the inside of your body), along with a review of your symptoms and health history. Treatments differ based on whether your diverticulitis is considered complicated or uncomplicated:
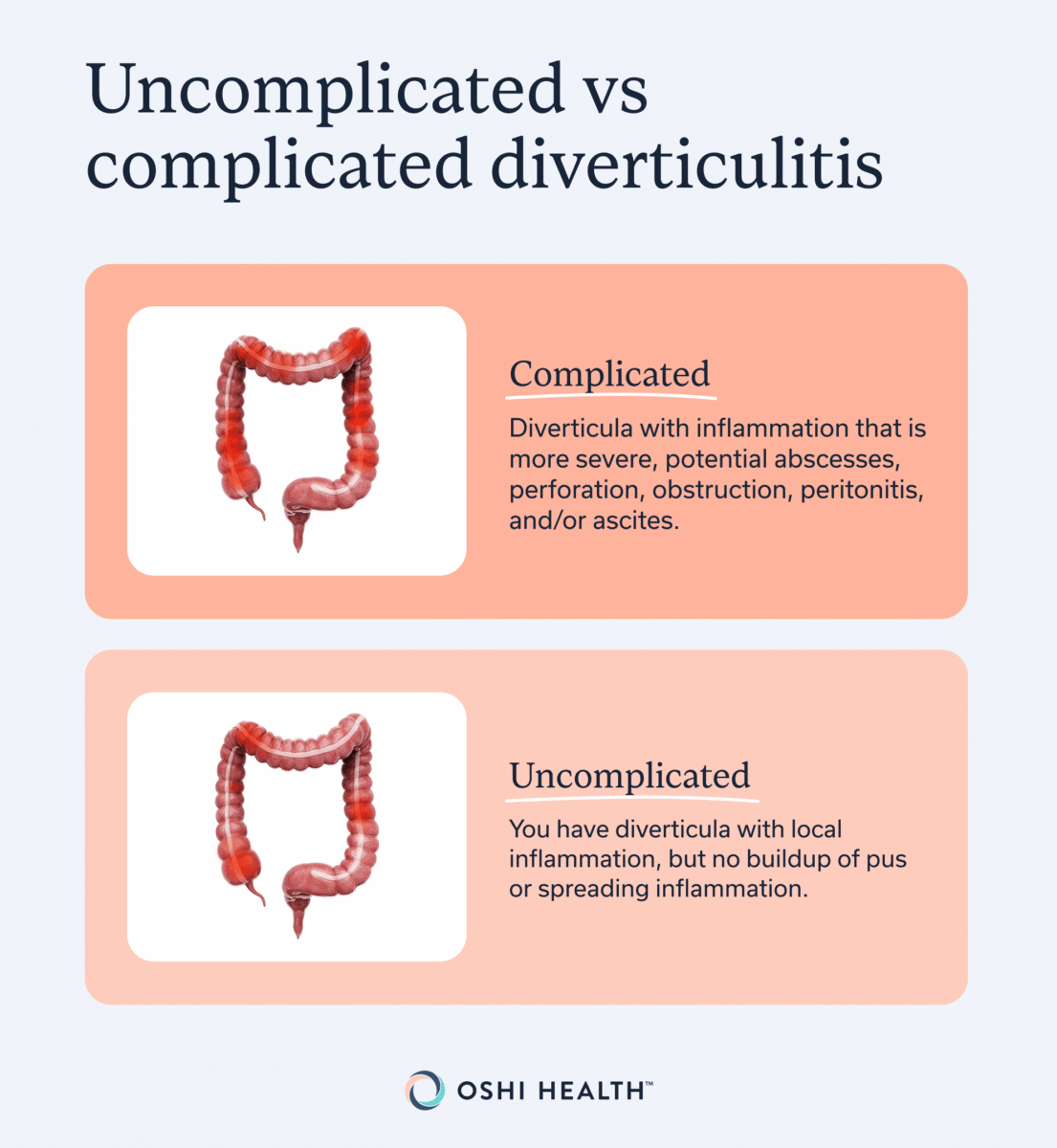
- Complicated: You have diverticula with inflammation that is more severe or spread out, as well as potentially abscesses (pockets of pus), perforation (intestine wall has torn), obstruction (blockage in the intestine), peritonitis (infection in the inner lining of your abdomen), ascites (fluid build-up in your abdomen), and other complications.
- Uncomplicated: You have diverticula with local inflammation, but no build-up of pus or spreading inflammation.
To put this into context, about 80% of people have uncomplicated diverticulitis, whereas only 20% have the complicated type.
Clinicians also classify the severity of diverticulitis to help them determine if you might need surgery. The most common staging system is the Hinchey classification, which is a four-stage, CT scan-based system.
Lower Hinchey stages, such as when someone has uncomplicated diverticulitis (stages 0 and 1a), can be treated medically and often without antibiotics.
Higher Hinchey stages, which are given when someone has large abscesses, bowel perforation, or peritonitis, indicate the potential need for surgery.
Antibiotic for diverticulitis: Who still needs them (and who may not)?
One of the biggest changes in modern diverticulitis treatment is that clinicians are much more selective about who gets antibiotics and who doesn’t.
“Historically, antibiotics have been the mainstay of diverticulitis treatment,” says Dr. Strate, “but there were no data to support their use.”
Over the past 20 years, high-quality evidence has stacked up to show that people with left-sided, uncomplicated diverticulitis can be treated safely and effectively without using antibiotics. (In non-Asian countries, the vast majority of diverticulitis cases occur on the left side).
These days, guidelines from the American Gastroenterological Association (AGA) and other health bodies state that most people with uncomplicated diverticulitis, who are otherwise healthy, should be managed without antibiotics.
However, antibiotics are still recommended for certain groups. You may be prescribed antibiotics for diverticulitis if you have complicated diverticulitis (Hinchey classifications II through IV), or if you’re at higher risk of complications due to having:
- A weakened immune system
- Allergies
- Chronic kidney disease
- High blood pressure
- Medical frailty
- Signs of sepsis
Diverticulitis surgery: evolving approaches and when it’s considered
There have also been recent developments in diverticulitis surgery: who gets it, who doesn’t, and what types of surgery are available.
Previously, surgery was automatically recommended after two uncomplicated diverticulitis “attacks,” and after only one attack for people under 40 years old. This is because subsequent attacks were believed to be more severe. However, recent evidence contradicts this.
“More recent studies found that complications of diverticulitis tend to happen during the first few episodes,” says Dr. State. Contrary to what was previously believed, diverticulitis severity actually decreases with each recurrent episode, and this pattern is similar across all age groups.
“Based on these findings, the number of diverticulitis episodes and patient age no longer dictate surgical intervention,” explains Dr. Strate.
Today, the approach to surgery is much more individualized and is based on a combination of factors, including:
- Impact of diverticulitis on the person’s quality of life
- Patient preference
- Surgical risks
Surgery for diverticulitis is rarely required these days. To put this into perspective, only 5% of people with diverticulosis go on to develop diverticulitis. And, of the 20% of people with diverticulitis who have complications, about 80% heal well after a few weeks of antibiotics, whereas 20% require surgery. Even though it’s uncommon, diverticulitis surgery can be life-saving in certain cases.
Changing surgical methods
Surgical methods for complicated diverticulitis have also evolved over the years. Instead of “open” surgery, in which a large cut is made on your abdomen, most surgeons use minimally invasive techniques, like laparoscopy and robotics, if possible. This involves tiny incisions through which a camera and small tools (either handled directly by your surgeon, or with a high-tech robotics machine) are inserted.
“In general, robotic approaches to surgery for diverticulitis are increasingly used,” says Dr. Strate. This surgical technique can:
- Improve visualization during the operation
- Minimize the number and size of incisions
- Reduce complications
Procedures that can prevent or delay surgery (complicated cases)
If you have complicated diverticulitis, then your GI provider may try less-invasive procedures before recommending surgery.
Abscesses that are larger than 3 centimeters (cm) are often treated with antibiotics and percutaneous drainage, which is when a small tube is used to drain fluid. Your provider will use imaging (like a CT or ultrasound) to guide them during the procedure.
Microbiome-based “new” treatments: what to know right now
Your microbiome refers to the community of bacteria, fungi, and viruses that naturally inhabit your gut. Everyone has a microbiome, but studies show that the microbiome of people with recurrent diverticulitis is significantly different from the microbiome of people without diverticulitis.
For that reason, researchers are looking into diverticulitis treatments that focus on the microbiome. However, take a pause before you drop some cash on pricy bottles of probiotics at your local health food store. Most of this research is still in its early stages.
“The gut microbiome is extremely complex, and what constitutes a ‘healthy’ microbiome in general—and for any given condition—is elusive,” says Dr. Strate. As you might imagine, manipulating a system with trillions of bacteria and thousands of species comes with its challenges.
“There is no good evidence that probiotics benefit patients with a history of diverticulitis,” says Dr. Strate. “And published guidelines do not recommend probiotics for diverticulitis management.”
Another microbiome treatment that’s under review is called fecal microbiota transplant (FMT), which involves the microbes from healthy donor stool being taken as a capsule.
However, there are only a few case reports (studies of a single person) that show FMT can prevent recurrent diverticulitis. “Currently, this could be regarded as an off-label, experimental use of FMT,” says Dr. Strate. However, there are two randomized trials under development, so keep an eye out for developments in the future.
CALLOUT BOX: Colonoscopy is often advised six to eight weeks after an episode of diverticulitis resolves, to rule out colorectal cancer or colitis. The exact recommendations for colonoscopy depend on factors like whether your diverticulitis is complicated or uncomplicated, how it was treated, when your last colonoscopy was, and other symptoms you might have.
Preventing diverticulitis with diet and lifestyle: what’s supported vs still emerging
It’s important to emphasize that, after your first episodes, future attacks of diverticulitis tend to be uncomplicated or less severe. “This information may be reassuring to patients with diverticulitis,” says Dr. Strate.
That said, there are still some lifestyle changes you can make to lower your risk of diverticulitis or prevent it from recurring.
According to Dr. Strate, certain eating patterns may reduce the risk of diverticulitis.
In the past, it was thought that seeds, nuts, and popcorn could aggravate diverticula and lead to diverticulitis. As such, people with diverticulosis were told to avoid these (and other fiber-filled) foods. What we know now is much different. Seeds, nuts, and popcorn are not, in fact, associated with diverticulitis, and diets high in fiber are actually very beneficial.
These days, people with diverticulitis are advised to eat diets high in:
- Fruits
- Legumes
- Nuts and seeds
- Vegetables
- Whole grains
To reduce recurrent episodes of diverticulitis, you should also avoid:
- Processed foods
- Red meat
- Unhealthy saturated fats
In addition to changing your diet, other lifestyle habits can also reduce diverticulitis recurrence:
- Avoiding NSAIDs, opiates, and steroids (unless prescribed for another condition)
- Avoiding or quitting smoking
- Reducing alcohol, especially liquor
- Maintaining a healthy body weight
- Regular physical activity
“Diverticulitis is an opportunity and motivation to improve one’s diet and lifestyle,” says Dr. Strate. However, this isn’t to say that having diverticulitis is your fault, or that it’s 100% down to lifestyle. Genetic factors are also at play, and scientists are trying to understand more about this.
However, regardless of your family history or genetic risk, a healthy lifestyle is beneficial and can also reduce the risk of other chronic diseases like cardiovascular diseases, diabetes, and cancer.
Working with a healthcare provider: building a plan you can actually follow
If these diet and lifestyle changes sound overwhelming, consider making an appointment with a dietitian or GI provider at Oshi Health. Together, you can chat about how to prevent diverticulitis recurrence in a manageable way that’s tailored to your current life.
The multidisciplinary GI team can also help if you’re experiencing a flare-up of diverticulitis by providing advice on:
- Management for constipation or diarrhea
- Recommended pain relief for diverticulitis (and what to avoid)
- Tips for keeping hydrated
- What to eat in the early days of a flare (such as when to opt for clear liquids and soft or bland food, and how to reintroduce more fibrous foods)
- When to head to urgent care or the emergency room
Medicine for diverticulitis: symptom control during a flare
Your clinician may prescribe certain meds to help your symptoms, like pain or nausea.
It’s especially important to talk to your provider about which pain relievers are recommended (or not) before you gulp down whatever over-the-counter pills are already in your medicine cabinet at home.
Non-steroidal anti-inflammatory drugs (NSAIDs)—which include common meds like ibuprofen, aspirin, and naproxen—are not advised for people with diverticulitis. This is because they can irritate your gastrointestinal (GI) tract and increase the chance of certain complications, including intestinal perforations. Your clinician may recommend alternatives, like acetaminophen or antispasmodics.
When to seek care: red flags you shouldn’t wait on
In some cases, diverticulitis can be an emergency. Head to the emergency room or urgent care if you have the following symptoms:
- Dizziness, weakness, or fainting
- High fever or chills
- Large amount of blood in stool
- Nausea or vomiting
- Rigid abdomen
- Severe or worsening abdominal pain
- Trouble keeping fluids down
For people who are pregnant or immunocompromised, consider seeking urgent evaluation at the very first sign of a red flag.
The Takeaway
- New treatments for diverticulitis are more personalized, less aggressive, and more evidence-based.
- Antibiotics are no longer given to everyone with diverticulitis. Most people with uncomplicated diverticulitis will not be prescribed antibiotics. They’re reserved for complicated or high-risk cases.
- Surgery for diverticulitis is no longer recommended after a benchmark number of episodes, because we know that severity decreases with recurrent episodes. Instead, it’s recommended based on personal risk and preference. Current surgical methods are also less invasive.
- Clinicians now consider the prevention of diverticulitis—through a fiber-filled diet, exercise, quitting smoking, and more—an essential part of care.
After more than 24 years of struggling, I finally received the care and attention I have been seeking for so long with Oshi. I cannot thank you all enough for how you have helped me get my life back!
— Zoe D.
Frequently Asked Questions (FAQs)
What gives immediate relief for diverticulitis?
Nothing gives immediate relief from diverticulitis; however, taking recommended painkillers (not NSAIDs), using a heating pad, resting, and sometimes a liquid or bland diet can help if you’re recovering at home.
How long does it take for the colon to heal from diverticulitis?
It could take one to two weeks to recover from a flare-up of uncomplicated diverticulitis. More complicated cases that require drainage or surgery could take longer to recover from.
Why are so many people getting diverticulitis?
The increase in diverticulitis incidence in Western countries is largely due to unhealthy lifestyle habits (like lack of exercise or smoking) combined with the availability of processed foods and diets low in fiber.
How can I beat diverticulitis without antibiotics?
The vast majority of people with uncomplicated diverticulitis can recover well without antibiotics. These days, antibiotics are typically only recommended in cases of complicated diverticulitis (when you have an abscess or widespread inflammation), or if you’re at high risk of developing complications, for example, due to being immunocompromised.
What is the new NICE procedure for diverticulitis?
One surgical technique that you might have heard of is the Natural Orifice Intracorporeal Anastomosis (NICE) technique, in which the diseased portion of your colon is removed through the rectum, rather than through a separate incision in your abdomen. “This is particularly useful in patients with a high body mass index, because body weight is a risk factor for surgical complications, including an infection of the abdominal incision site,” explains Dr. Strate.
Oshi is your partner in digestive health
Feel like your digestive concerns are running your life? You’re not alone—and we’re here to help you find lasting relief.
Oshi Health GI providers, gut-brain specialists, and registered dietitians work together to address your symptoms and find solutions that actually work for you.
Whether you’re dealing with chronic digestive issues or unpredictable symptom flare-ups, our GI specialists deliver:
✔ Personalized care plans tailored to your lifestyle
✔ Science-backed strategies to calm your gut
✔ Compassionate, whole-person care
✔ And so much more!
Ready to take control of your gut health?